Lung Cancer Answers is a website devoted to life issues for lung cancer patients and their families and is sponsored by Brad Cooper* of Cooper, Hart, Leggiero & Whitehead, PLLC. Cooper, Hart, Leggiero & Whitehead is located in The Woodlands, Texas (Greater Houston Area), handles cases nationwide with co-counsel in state of filing, and can be reached toll-free at 1-800-998-9729 for more information on lung cancer. Brad Cooper is not a medical doctor. The information on these pages is for the education of lung cancer patients and their families regarding potential medical and legal options. Patients are advised to consult with a medical doctor.
* Licensed by the Supreme Courts of Texas.
Symptoms and the results of imaging tests may strongly suggest that a patient has lung cancer, but the actual diagnosis of cancer is dependent on obtaining tissue samples that can be analyzed under a microscope. The role of surgery in the management of lung cancer is twofold – first to acquire the tissue to be analyzed through a biopsy procedure, and second, to treat the cancer by surgical removal in selected patients.
Surgical Procedures to Diagnose Lung Cancer
If a lung mass is seen on imaging tests, one or more of the following procedures may be performed:
Bronchoscopy
In a bronchoscopy procedure, the physician inserts a thin, flexible, lighted tube called a bronchoscope through the nose or mouth and into the trachea (windpipe) and bronchi (airways). Through this tube, the surgeon can examine the inside of the trachea, bronchi, and lung and can, at the same time, collect small tissue samples. The doctor can also obtain cells from the lining of the airways with a small brush (bronchial brushing) or by rinsing the airways with sterile saline (bronchial washing).
Fine Needle Aspiration Biopsy
In a fine needle aspiration biopsy, the doctor guides a thin, hollow needle into the area while looking at the lung with either fluoroscopy (similar to an x-ray, except the image is shown on a screen) or CT scans. A small sample of the mass is then sucked into a syringe and sent to the lab for analysis. If a diagnosis is inconclusive due to the limited size of the tissue sample taken, a larger needle may be used to obtain a slightly larger piece of tissue. This is called a core needle biopsy.
Endobronchial Ultrasound
In this procedure, a bronchoscope is fitted with an ultrasound transducer at its tip and is passed down into the windpipe. The transducer can be pointed in different directions to look at lymph nodes and other structures in the mediastinum (the area between the lungs). If suspicious areas are seen on the ultrasound, a hollow needle can be passed through the bronchoscope and guided into these areas to obtain a biopsy. Because lung cancer frequently spreads to lymph nodes in the mediastinum, biopsies of this area are often necessary.
Endoscopic Esophageal Ultrasound
This technique is similar to endobronchial ultrasound, except the doctor passes an endoscope (a lighted, flexible scope) down the throat into the esophagus. The esophagus is located just behind the windpipe and is close to some lymph nodes in the chest where lung cancer may spread. Ultrasound images are then taken from inside the esophagus to determine whether there are enlarged lymph nodes that could contain cancer. If these lymph nodes are identified, a hollow needle can be passed through the endoscope to obtain samples.
Mediastinoscopy
In this procedure, a small incision is made at the front of the neck and a thin, hollow, lighted tube is inserted behind the breast bone and in front of the windpipe to visualize the area. Special instruments can then be passed through the tube to take tissue samples from the lymph nodes along the windpipe and the major bronchial tube areas. A complete procedure includes an extensive sampling of lymph nodes in the upper and lower mediastinum.
Thoracoscopy
In this procedure, a small incision is made in the side of the chest wall. The doctor then inserts a lighted tube with a video camera on the end through the incision in order to view the space between the lungs and the chest wall. If suspicious areas are seen, tissue samples can be taken. If certain areas cannot be reached with thoracoscopy, the surgeon may need to make a larger incision in the chest wall. This is called a thoracotomy. In a thoracotomy, there is direct access to the mass, and the surgeon is able to remove part or all of the suspicious area.
Thoracoscopy may also be used in surgical treatment to remove part of a lung in some early-stage lung cancers. This type of procedure is known as “video-assisted thorascopic surgery” or VATS.
Thoracentesis
A thoracentesis is a procedure done to determine if a build-up of fluid around the lungs, called a pleural effusion, is the result of cancer that has spread to the pleura (lining of the lungs). In this procedure, a hollow needle is inserted between the ribs to drain the fluid. The fluid is then checked for cancer cells under a microscope.
Surgical Procedures Used to Treat Lung Cancer
Surgery to remove the lung cancer may be an option for some early-stage non-small cell lung cancer patients, and for those who are candidates, it may provide the best chance for a cure. That said, the trend today is that surgery is combined with other treatment modalities to help ensure that any microscopic disease is eliminated thereby reducing the likelihood of recurrence.
Since surgery for lung cancer is complex and can have serious consequences, it is important for patients to carefully evaluate benefit versus risk. It is also important that the surgeon chosen is experienced in the various types of surgery used for lung cancer, and is able to communicate with their patient regarding any questions or concerns they may have. General surgeons perform all types of surgery, but may not have specialized training in lung surgery. Thoracic surgeons have received specialized training in lung surgeries but also specialize in cardiac (heart) surgeries. The best possible choice would be a thoracic surgeon that specializes in lung surgeries.
Surgical resection is often recommended when the cancer has not spread to other tissues in the chest or elsewhere in the body. It may be the first type of treatment received, or it may be done after other treatments such as chemotherapy or radiation have been given to shrink the tumor before surgery.
Surgery is not generally recommended as first-line therapy if:
- The cancer has spread to the opposite lung
- The cancer has spread from the lung into other structures in the chest
- The cancer has spread to lymph nodes in the neck or to distant sites in the body such as the liver, brain, or adrenal glands
- The cancer has developed in an area of the lung where removal is impossible
- The cancer has been diagnosed as small cell lung cancer
Surgery is not recommended for those who have other concurrent health problems such as heart disease or diabetes that would make the surgery too risky.
The type of surgery the doctor recommends depends on several factors including the size and location of the tumor and the patient’s level of lung function. In some cases, if the patient’s lungs are healthy enough, the doctor may choose to perform more extensive surgery to provide a better chance for a cure.
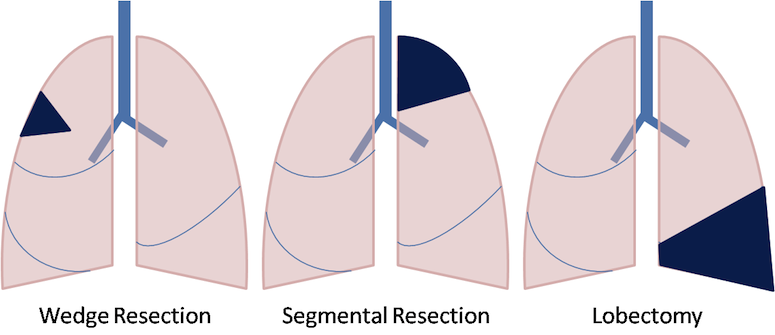
The three types of surgery most often used for lung cancer are:
- Wedge Resection. A wedge resection is a surgical procedure that removes a small, wedge-shaped portion of the lung along with healthy tissue surrounding the area. A wedge resection is performed instead of a lobectomy when there is a danger of decreased lung function if too much of the lung is removed. This surgery can be performed by minimally invasive video-assisted thoracoscopic surgery (VATS) or a thoracotomy (open chest surgery).
- Segmentectomy. A segmentectomy, or segment resection, is a surgical procedure that removes a larger portion of the lung lobe than a wedge resection but does not remove the whole lobe. This surgery is preferred when the patient’s lung function would be too compromised by removing an entire lobe of the lung (lobectomy). The risk associated with the return of the cancer is higher with this method.
- Lobectomy. In this procedure, the surgeon removes an entire lobe of the lung containing the cancer. The right lung has three lobes and the left lung has two lobes, and the lungs are capable of functioning with the lobe(s) that remain. The removal of two lobes is called bilobectomy. You can read more on the lobectomy procedure here.
Another, less common type of surgery performed on patients with lung cancer is a pneumonectomy. A pneumonectomy is a surgical procedure in which an entire lung is removed, in most cases, for cancer of the lung that cannot be treated by removal of a smaller portion. This surgery requires an open chest technique (thoracotomy). A pneumonectomy is done only when necessary because it greatly reduces overall lung function.
All of these procedures are done under general anesthesia, with access to the chest cavity via a surgical incision called a thoracotomy. Some doctors, however, prefer to treat selected early-stage lung cancers located near the outside of the lung with a procedure called video-assisted thoracoscopic surgery or VATS, which is less invasive than a thoracotomy. In this procedure, a thin, rigid tube with a video camera on the end is placed through a small incision in the side of the chest to help the surgeon see the chest cavity on a TV monitor. One or two additional incisions are made, and instruments are passed through these openings to perform the same surgical procedure that would be done using a thoracotomy. If a lobectomy or pneumonectomy is necessary, one of the incisions is enlarged to accommodate the specimen being removed. Because the incisions are significantly smaller than with thoracotomy, the patient experiences less surgical pain and a shorter hospital stay.
All medical procedures carry some risk, and complications during and after surgery may be influenced by the patient’s overall health status prior to the surgery, and the extent of the surgery. Serious complications may include pneumonia, infection, or excessive bleeding. In rare cases, patients may not survive. Recovery time may vary; the typical time frame is weeks to months.
Read more about:
» Treatment of Lung Cancer
» Lung Cancer Prognosis
» Lung Cancer Patient Assistance
If you, or someone you know, has lung cancer and you would like to know if they qualify for additional compensation, please call 1-800-998-9729 for a FREE consultation.
©2026 Cooper, Hart, Leggiero & Whitehead, PLLC. All rights reserved.